
Upper limb pain is very common. Every person will face this problem throughout their life. This is due to the fact that a person makes a lot of active movements in the arms and shoulder girdle daily. In most cases, pain in the upper extremities is the result of excessive stress on the stabilizing structures – ligaments, tendons, joint capsules (static), and dynamic muscles, as well as a sports injury or fall, which can result in dislocation and subluxation, fractures. However, it can also occur after sudden movements in daily life, as a result of poor posture, muscle imbalance, reduced blood flow, or soft tissue imbalance.
Symptoms of an upper limb damage may vary depending on the location of the problem. In general, symptoms such as:
-
Sensitivity in the affected area
-
Localized redness and swelling
-
Pain in the joints
-
Decreased freedom of movement in the limb
-
Paresthesia – feelings of tingling and crawling. Such a feeling occurs when a nerve is involved in the pathological process, for example, squeezing as a result of edema.
When we talk about pain in the arm, we do not specify the location of the pain. In fact, the upper limb of a person consists of several regions, pain in each of which can be caused by its own causes. Let us dwell further on the anatomy of the upper limb.

Anatomical features of the upper limb
The upper limb consists of two parts: the girdle of the upper limb and the free part of the upper limb. The girdle of the upper limb or shoulder girdle consists of the scapula and collarbone, which are interconnected by muscles, ligaments and joints. The shoulder girdle provides high mobility of the upper limb, which is why in case of a fracture, for example, of the right clavicle, the patient’s right arm completely loses the ability to move.
The shoulder girdle is directly connected with the thoracic spine, which means it is of great importance in the formation of posture. This is due to the fact that, unlike the girdle of the lower extremities, the scapula and collarbones are not rigidly fixed to any anatomical structures, but are, as it were, “suspended” on the muscles and ligaments to ensure maximum mobility. In addition, the shoulder girdle is a fixing structure for the cervical spine. Thus, in case of muscle imbalance, as, for example, occurs with the upper crossed syndrome (UCS), the shoulder girdle is one of the first involved in the process of changing posture: with a round back, the shoulder blades seem to move apart from each other, the shoulders and neck move forward, and the thoracic region the spine is flexed. Strengthening the muscles of the shoulder girdle is of great importance, because, as you know, posture disorders and upper crossed syndrome are fraught with problems such as chronic pain, respiratory failure (the shoulder girdle is directly connected to the chest), reduced freedom of movement, etc. The free part of the upper limb consists of three sections: shoulder, forearm and hand..
the Shoulder & shoulder joint
The shoulder begins at the shoulder joint – the place where the upper limb is attached to the shoulder girdle. The “skeleton” of the shoulder joint is formed from the scapula, collarbone and humerus. These bones are connected to each other by four joints – sternoclavicular, acromioclavicular, humeroscapular and scapular-thoracic. As you can see, the shoulder joint consists of four anatomical structures, each of which should work in harmony with the others and maintain their functions in order to provide movement. The bones of the shoulder joint are fixed and controlled by 19 muscles. The muscles of the shoulder are divided into two groups: external (they help to move the shoulder girdle and shoulder relative to the axial skeleton) and internal (movement relative to the scapula). Together, the bones, tendons, and muscles of the shoulder (a group of stabilizing muscles) make up the rotator cuff, which allows the arm to be raised and rotated. Inside the cuff, there are small sacs filled with synovial fluid called bursae. The bursae act as “pillows’ to help reduce friction during movement between the elements of the joint—mainly the bony structures and tendons..
The shoulder joint is a complex system elaborated by the nature, which, nevertheless, is subject to frequent microtraumas as a result of daily activities, heavy lifting, sudden movements. Pain that occurs in the area of the shoulder joint may vary, depending on the cause that caused them, but they certainly increase with movement – abduction, rotation of the arm in the joint.
To understand the complex biomechanics of the shoulder joint, you should understand that for a simple movement in the shoulder – raising the arm – a well-coordinated, coordinated work is required not only from the four main components (sternoclavicular, acromioclavicular, shoulder-scapular and scapular-thoracic joints), but also with stability and mobility provided by the thoracic and cervical spine, as well as the correct posture and stability of the pelvic girdle, with which the shoulder is connected through the latissimus dorsi muscle. Thus, the movement in the shoulder-scapular joint is accompanied by the movement of the clavicle and scapula (scapular-shoulder rhythm), extension of the thoracic region and retraction of the cervical spine, the activation of 4 stabilizing muscles (rotator cuff), which strengthen the head of the humerus in the joint, requires proper volume joint capsule and the strength of the ligamentous and muscular apparatus. As well, all this is required to maintain the clearance (gap) between the acromion and the head of the humerus, which is necessary for full articular movement. In the case when, for various reasons, there is a narrowing of this lumen, the so-called impingement syndrome may develop, which is the most common cause of the development of pain and dysfunction of the shoulder joint. More details will be described below.
Elbow joint
Between the shoulder and forearm, there is a small area – the elbow joint. This joint is formed by three bones – the distal end of the humerus on one side and the proximal parts of the ulna and radius on the other. The mobility of the elbow joint is quite wide, and the load on it in everyday life is no less than on the shoulder joint.
We use the elbow joint in weight lifting, sports training and many other activities. The complex structure of the joint with many ligaments and articular surfaces, combined with its frequent use in everyday life, leads to an increased risk of injury. For example, one of the most common injuries affecting about 3% of the total population is the so-called “tennis elbow”. In fact, this condition occurs not only in professional athletes (such cases make up only 5% of the total): “tennis elbow” occurs in people who, for work or a hobby, often make repetitive movements in the elbow joint. We will return to this disorder below.
Forearm
The forearm, as we already know, is located below the elbow joint and consists of two bones: the ulna and the radius. In the forearm, as well as in the shoulder area, there are many muscles designed to provide precise movements and fine motor skills. In the distal part of the arm, the forearm is connected to the hand with the help of the wrist joint. Fractures of the forearm bones occur quite often: according to some studies, the frequency of such injuries reaches 30% of the total number of fractures. Such statistics are mainly due to fractures resulting from a fall: when falling, a person usually puts his hands forward, as a result of which the main load from the impact falls on the limb, in particular, on the forearm. There is an axiom: a fracture of one of the paired bones, especially with a displacement, is usually accompanied by a fracture or dislocation of the other. Since the bones in the forearm are paired, injuries usually also affect both bones.
the skeleton
The skeleton of the hand consists of eight short bones of the wrist, bones of the metacarpus, phalanges of the fingers, as well as many muscles, joints, blood vessels and nerves. The hand performs complex functions – sensory and motor, is constantly used in life, and therefore is subject to traumatization.
The pathological process and, as a result, limitation of movement in any of the above structures will adversely affect the biomechanics of the upper limb, and therefore, if any injury or pain occurs, you should immediately contact a specialist.
It’s important to know!
Pain in the upper limb can be caused not only by injuries and direct damage to the musculoskeletal system in this area. In some cases, PAIN IN THE LEFT ARM, combined with changes in PULSE, excessive SWEETING, Difficulty BREATHING, NAUSEA and other symptoms, may be a sign of a myocardial infarction. If you suspect a cardiac cause of the pain, you should immediately consult a physician


Possible causes of the upper limb pain
Disorder of the shoulder
Damage to the shoulder joint
As we already know, the damage to the shoulder joint is quite common. Due to the complex structure, fairly loose joint capsule and wide range of motion, injuries in its area are not uncommon. In some cases, constant tension or excessive load for a long time in the area of the shoulder joint can lead to inflammation and swelling of the tendons inside the rotator cuff, inflammation of the periarticular bag, tear and complete rupture of the tendons, development of shoulder instability. As a result, there is a painful condition, an inflammatory process and, as a result, a limitation of articular movements and an impairment of the daily function of the upper limb.
Impingement Syndrome
As already described – is the most common disorder contributing to the development of pain and dysfunction of the shoulder joint.
A condition in which there is a muscular imbalance in which the tendon ne shoulder muscles, mainly the rotator cuff, are “pinched” by a ligament or bone due to a decrease in the subacromial space. This condition, which is most common in people 35 years of age and older, can cause pain in the front or back part of the shoulder.
What is the disorder? Repetitive injury to the rotator tendons can develop during shoulder elevation when friction and pinching occurs, including pinching of other soft tissues.
This repetitive rubbing damages tissues and causes local inflammation, tendinitis and bursitis (including pain), which is the cause of functional impairment and can lead to degeneration, tearing and even their complete rupture. tendons and muscles,
Functional impairment of the stabilizing muscles of the shoulder can cause impaired stabilization of the shoulder and exacerbate injury and joint instability
The main causes for the syndrome development are:
-
Incorrect posture, problems of the cervical and thoracic spine with damage to the nerve roots that innervate the muscles of the shoulder and arm (including the rotator cuff)
-
Incorrect position of the shoulder and scapular-costal joints and, as a result, a change in the biomechanics and coordination of the movement of the constituent components of the shoulder girdle when raising the arms
-
In most cases, it manifests itself against the background of repeated loads on the shoulder muscles, as a result of which their stabilizing insufficiency develops.
Shoulder bursitis

Bursitis is an inflammation of the periarticular bag, which can be infectious and aseptic in nature.
Aseptic bursitis occurs when the shoulder joint is constantly overloaded and subjected to microtrauma. The cause for the condition is often the mode of operation: bursitis is often found in loaders and athletes. Less commonly, bursitis can develop as a result of a single injury.
Normally, the periarticular bursa produces synovial fluid, which is necessary to reduce friction in the joint. With constant trauma and high load, friction increases, the periarticular bag becomes inflamed and begins to produce a large amount of synovial fluid. As a result, edema develops and pain appears.
Aseptic bursitis is characterized by moderate pain in the shoulder area, redness and slight swelling. Passive and active movements are limited in the joint, “clicking” sounds may occur when trying to move. Bursitis can end in recovery or become chronic.
Risk factors for the disease development include:
-
Elderly age
-
History of rotator cuff tendon injury
-
Increased load on the shoulder joint in work or hobbies
-
Incorrect posture or lifting technique
-
Lack of stretching before training.
Shoulder tendinitis
Tendonitis is an inflammation of the joint tendons, which occurs more often as a result of high loads, sports, hypothermia. Most often, tendinitis of the shoulder joint occurs in tennis players, basketball players, volleyball players and gymnasts. With this pathology, pain occurs when performing certain movements: when the patient reaches out to take something, throws his hand forward, performs sharp movements above his head. Over time, the pain appears at rest and even “radiates” to the area of the elbow joint.
Externally, mild edema may be present. Over time, with the progression of the disease, joint contracture is formed – a steady decrease in its mobility, sometimes complicated even by a “frozen shoulder” – or “capsulitis”. This is a condition in which the patient complains of pain in the arm and limited range of motion of the shoulder.
It is caused by long-term inflammation that causes stiffness and limited movement of the shoulders and can also cause difficulty in daily activities.
Common risk factors for development of the disease include:
-
Poor posture, stoop, upper crossed syndrome (UCS)
-
Tension of the muscles of the shoulder girdle
-
Weakness or imbalance of the shoulder muscles
-
Neurological causes of pain in the shoulder joint
Diseases of the cervical spine
Often, pain in the shoulder joint can be triggered by diseases of the cervical spine, such as:
-
osteochondrosis;
-
intervertebral hernia;
-
spondylitis;
-
spondylarthrosis;
-
deforming spondylosis;
-
spinal stenosis.
In diseases of the spine, the height of the intervertebral disc often decreases, the structures begin to compress the roots of the spinal nerves, which can result in chronic pain.
Pain radiating to the shoulder joint is usually sharp, “shooting”, the pain can spread to the entire arm, to the fingertips. Pain associated with the cervical region is easy to distinguish from pain in the pathology of the joint itself – movements in the shoulder with neurological pain are not limited.
Traumatic injuries
Traumatic injuries are common causes of pain in the shoulder joint.
When the shoulder joint is injured, a moderate, quickly subsiding pain, the function of the limb is preserved, but the movements are limited, the patient with a bruise “protects” the affected limb.
A dislocation of the shoulder joint is characterized by a very sharp pain in combination with a click. Until the joint is repositioned, the pain remains intense, the joint itself is visually deformed, movements in it are impossible.
Humeral head fractures are characterized by severe pain that does not subside with time. Movements in the joint are dramatically limited, the patient holds the limb, in order to avoid the formation of pain. At the same time, a strong edema, cyanosis is determined, deformation of the limb, pathological mobility, crepitus are visually possible.
Degenerative changes
Degenerative changes in the shoulder joint can also cause pain. Arthrosis of the shoulder joint is characterized by chronic pain, which is localized, as it were, in the depth of the joint. Over time, the pains intensify, their intensity increases, they appear more often and significantly affect the quality of life. The pain often occurs at night, the limitation of mobility in the joint gradually increases.
Disorder of the elbow joint
The most common disorder that causes pain and limited mobility in the elbow joint is “tennis elbow”. It develops as a result of overstrain of the elbow joint, more often as a result of prolonged repetitive performance of monotonous movements. Pain most often occurs on the outer part of the elbow and may be accompanied by swelling, redness, and localized fever. In the evening and at night, the pain becomes more pronounced. In this condition, the elbow retains its full range of motion as the internal joint is not affected.
Tennis elbow is traditionally treated with a combination of physical therapy, application of cold to the affected area, non-steroidal anti-inflammatory drugs, and rest. In some cases, a forearm brace is used to “force” the affected tendons to rest.
Disorder of the forearm
Fractures are especially characteristic of the forearm region, because it is this region of the human body that often takes on most of the load during a fall. READ MORE
In traumatology, the following fractures of the bones of the forearm are distinguished:
-
Fractures of the radius in a typical location;
-
Fractures of the diaphysis (middle part) of both bones of the forearm;
-
Fractures of the ulna in its middle part (fractures of the diaphysis);
-
Fractures of the radius in its middle part (fractures of the diaphysis);
-
Fractures of the neck or head of the radius;
-
Montage fractures (fractures of the ulna in the upper third, combined with dislocation of the head of the beam);
-
Galeazzi fractures (fractures of the lower third of the radius, combined with dislocation of the lower end of the ulna and rupture of the peripheral articulation of the bones of the forearm).
-
Fractures of the olecranon;
-
Fractures of the coronoid process.
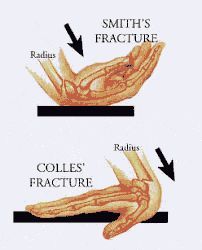

One of the most common fractures in the forearm is the Collis and Smith fracture – fractures of the radius in a typical location. This fracture is localized in the area of the wrist joint, 2-3 cm higher. The cause of such a fracture is a fall on a straight arm with an emphasis on the palm, less often on the back of the hand. With such an injury, cyanosis, swelling, and sharp pain are observed in the area. When nerves are involved in the process (the branches of the median and radial nerves pass in this area), sensitivity disturbances, restriction of movements of the fourth finger may occur.
Disorder of the wrist area

Speaking of pain in the upper limb, we should mention such a pathology as carpal tunnel syndrome (tunnel syndrome). This syndrome is formed as a result of compression of the median nerve by the bones and the transverse carpal ligament. This condition occurs as a result of monotonous flexion-extensor movements, among musicians, artists, and chiropractors. As a result of long-term maintenance of a non-physiological position of the hand or direct pressure on it, the median nerve is compressed, and sensitivity disorders occur, manifested by paresthesia, pain, weakness of the hand.
Video: “Rehabilitation of the upper limb disorders”
Upper limb. Set No.1 improvement of mobility and range of joint movement
For additional information about the rehabilitation of the upper limb disorders, you can watch a video demonstrating exercises and rehabilitation recommendations.
Treatment of the upper limb disorder
Diseases of the upper extremities are closely related to the spine region, cervical and thoracic region, connected with the upper crossed syndrome, and significantly affect daily activities. Properly selected treatment allows patients to improve the quality of life and return to activity without pain.
The most effective method of conservative therapy is physiotherapy, exercise therapy, manual therapy and massage. In some cases, special bandages and corsets are used. If the pain is caused by excessive tension, cool compresses and rest are prescribed, for more severe symptoms, non-steroidal and steroidal anti-inflammatory drugs are indicated.

Check the demo version of our sets of exercises for the Upper Limb Problems on YouTube
Our website presents the following sets of exercises for the upper limbs:



